Responding to Harassment and the Impact on Physician Wellness
By Anne L. Becker, MD
The elderly man approached me in the clinic hallway; pointed at my name badge; and said, “That says ‘Physician.’ You must have stolen that from someone!” As a woman physician, I am assumed to be not-a-doctor on a regular basis, and I felt a familiar swirling of emotions—confusion and disbelief, followed quickly by irritation and disgust—in response to his “joke.”
There is increasing awareness of the impact that microaggressions and mistreatment have on physician wellness (1). Mistreatment can happen to anyone in health care, but it is particularly harmful when it is focused on a person's unique characteristic or membership of a group that has a historical legacy of experiencing discrimination or othering. Examples include one's race, ethnicity, immigrant status, gender, gender identity, sexual orientation, religion, disability, or body size (2).
I was chatting about this with a Black physician colleague recently, and he effortlessly listed about a dozen personal examples of bias or harassment. One particularly egregious example involving outright verbal abuse and ridicule from a patient was made much worse, he said, because a physician who witnessed the exchange said nothing and did not intervene, causing him to feel helpless and alone (3).
The almost daily requirement to prevent and react and respond to these situations can lead to burnout and exhaustion on top of the existing challenges of practicing medicine. Certainly, the most effective interventions to address these issues occur at the institutional level (4). There must be change in our systems and policies in order to create equity and inclusion in hiring, retention, and promotion (5).
We know that this level of change takes time, so what can we do right now? How can we respond?
Prepare to Respond to Harassment in the Work Environment
The first step is to expect that harassment will occur to us or our colleagues. Knowing this allows us to prepare our response. When we witness or experience one of these scenarios, it is natural to freeze and not know what to say or to respond with the first emotion that comes to the surface—often anger.
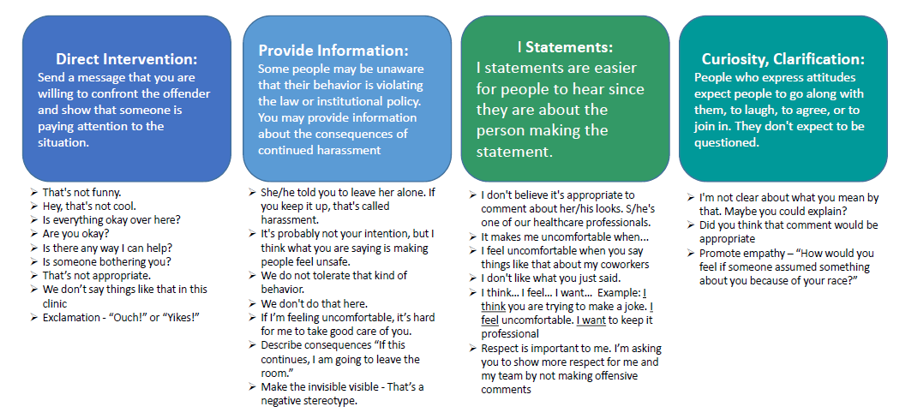
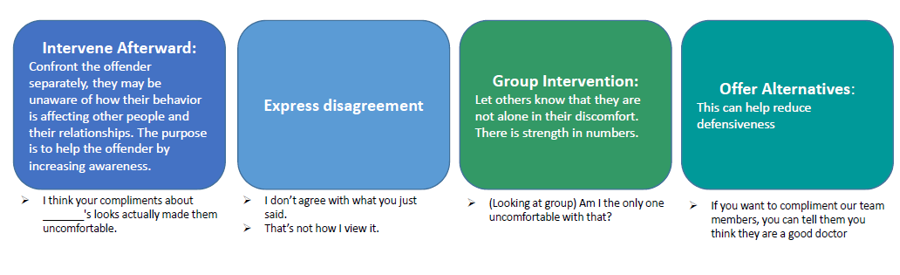
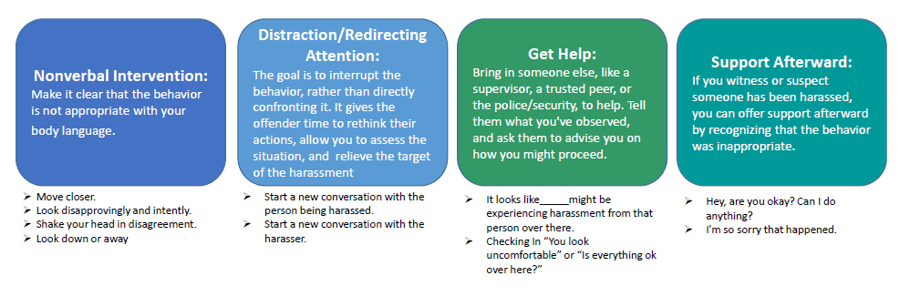
I learned about a versatile and practical toolkit available for learning how to respond to these stressful encounters from a University of Minnesota faculty development workshop called “Responding to Harassment in the Clinical Learning Environment; A Practical Workshop for Faculty,” which was created by a psychologist and two physicians from the Minneapolis VA (6, 7). The workshop shared a framework for how to take action before, during, or after a problematic encounter and provided a handout on bystander response (8). The importance and power of the bystander response resonated with me and helped me take real action when confronting harassment in the clinical learning environment. Check out the toolkit created from this handout below.
By having a toolkit of possible responses, we can feel empowered to do something for ourselves or act as an advocate and an ally for our colleagues. There are intentionally a broad variety of tools to choose from, because we all have different levels of comfort with conflict, assertiveness, and psychological safety—even within ourselves in different contexts.
Think of another emotional and unexpected situation, such as a Code Blue. We practice the words and actions of those events so that we have a familiar script to turn to in order to help us do what we need to do without having to invent something in a heated and unexpected moment.
For example, someone who is typically shy or reserved may have trouble with direct confrontation and could try one of the “Nonverbal Intervention” suggestions, such as shaking their head in disagreement. Another person who has a tendency to be too blunt could try an “I Statement,” such as “I feel uncomfortable when you comment on my appearance.” You should pick an example from the toolkit to try out and have it in your back pocket so you can pull it out in the moment without thinking about it. Teach your learners that harassment will happen and that it's important to be ready before it happens. Most important, if you do freeze in the moment, you can still seek or provide support by talking through it with a trusted colleague. If you witness something, you can debrief afterward by simply stating, “I'm sorry that happened. I didn't know what to say. Are you okay?”
If we don't prepare ourselves and our colleagues for workplace mistreatment, it can be disastrous for the physician. It can trigger strong emotions, outbursts, and unprofessional conduct that can damage not only the patient–physician relationship but also the physician's career and license (9). It is our duty as individuals, and within institutional systems, to support physicians in learning how to confront this (10).
In my case, I tend to keep the tool of “curiosity” in my back pocket. When the man in the clinic challenged my identity as a physician with a tacky “joke,” I countered by asking, “What do you mean?” He then stated that it was just a joke and that he thought I would laugh. I calmly and professionally told him that I didn't get it and asked him to explain it to me. He became a bit flustered; said, “Never mind.”; and walked away. I likely did not change that one person's worldview or tendency toward inappropriate comments, but I did feel more empowered after using my tools. In addition, the emotions of irritation and disgust were replaced with feelings of bravery and pride.
Response to Harassment Toolkit (2, 3)
References
- Barrett E, Salas M, Dewey C, et al. A call to action: align well-being and antiracism strategies. ACP Hospitalist. 15 March 2021. Accessed at https://acphospitalist.org/archives/2021/03/a-call-to-action-align-well-being-and-antiracism-strategies.htm.
- Paul-Emile K, Critchfield JM, Wheeler M, et al. Addressing patient bias toward health care workers: recommendations for medical centers. Ann Intern Med. 2020;173:468-73. [PMID: 32658573] doi:10.7326/M20-0176
- Paul-Emile K, Smith AK, Lo B, et al. Dealing with racist patients. N Engl J Med. 2016;374:708-11. [PMID: 26933847] doi:10.1056/NEJMp1514939
- Serchen J, Doherty R, Atiq O, et al; Health and Public Policy Committee of the American College of Physicians. Racism and health in the United States: a policy statement from the American College of Physicians. Ann Intern Med. 2020;173:556-7. [PMID: 32559145] doi:10.7326/M20-4195
- Price EG, Gozu A, Kern DE, et al. The role of cultural diversity climate in recruitment, promotion, and retention of faculty in academic medicine. J Gen Intern Med. 2005;20:565-71. [PMID: 16050848]
- Bemmels H, Ingraham K, Tiryaki E. Responding to Harassment in the Clinical Learning Environment: A Practical Workshop for Faculty. University of Minnesota Faculty Development Workshop. 2020. Corresponding author: Ezgi.Tiryaki@va.gov
- Bemmels H, Ingraham K, Tiryaki E. Responding to Harassment in the Clinical Learning Environment: A Practical Workshop for Faculty. Workshop Handout: Bystander Intervention Strategies. University of Minnesota Faculty Development Workshop. Minneapolis, MN.
- Shankar M, Albert T, Yee N, et al. Approaches for residents to address problematic patient behavior: before, during, and after the clinical encounter. J Grad Med Educ. 2019;11:371-4. [PMID: 31440327] doi:10.4300/JGME-D-19-00075.1
- Jain SH. The racist patient. Ann Intern Med. 2013;158:632. [PMID: 23588752] doi:10.7326/0003-4819-158-8-201304160-00010
- Youmans QR. The N-word. Ann Intern Med. 2019;171:380-1. [PMID: 31476228] doi:10.7326/M19-1269
Building Community, One Connection at a Time
By Kerri Palamara, MD, MACP
Our monthly coaching calls with Well-being Champions and Crissy Walter and Kierston Scott from ACP have become a bright spot in our calendars. Many who join us have found a sense of community and camaraderie in these groups, even if it is not the same faces each time. Knowing there is a place to go where you can be in community with others, receive support and encouragement, and walk away with action items has helped many champions fight back against the sense of loneliness that has crept in for many. We can't completely blame the COVID-19 pandemic for this—we were a lonely society in the United States before COVID-19, and the pandemic has introduced new ways to feel lonely.
So, what is this concept of loneliness all about? Loneliness is defined as “a person's feelings about the adequacy and quality of his or her relationships in particular situations” (1). Contrary to what you might think, loneliness can occur when you work alone or are surrounded by people. Think of a busy nursing station, buzzing with activity and people, and a doc sitting at a computer, alone with their feelings. Loneliness is impacted by the same stressors that drive burnout and affects 3 in 5 adults in America (2). Chronic loneliness can have serious consequences, such as anxiety, depression, and substance use disorder (1–3). The statistic that really changed my view on the importance of addressing loneliness was this: The chronic stress of loneliness can be as risky as smoking 15 cigarettes per day and increases your risk for heart disease by 29% (3)!
Loneliness can be a viscous cycle: When feeling lonely, one tends to withdraw emotionally and stop participating in social events, which only furthers isolation. For example, how many times have you heard a comment like, “Why should we invite Bob? He never comes to anything,” or, “Marie barely talks to anyone, I doubt she'd want to come.” The lonelier we become, the more we feel disconnected and insecure, self-doubt creeps in, and negative thoughts and ruminations become more persistent (2, 3). Those who experience loneliness in the workplace begin to disengage from the work itself and the organization, which can lead to loss of meaning and purpose, decreased productivity and creativity, and increased turnover (3).
If you aren't sure if you are lonely, the UCLA Loneliness Scale is a good place to start (4). U.S. Surgeon General Dr. Vivek Murthy helps us understand how to consider loneliness and its antithesis, connection, in his book Together: The Healing Power of Human Connection in a Sometimes Lonely World. He describes three levels of connections that sustain us: intimate (partner, spouse, best friend), or someone who knows you for who you truly are; relational (circle of friends), or people you want to spend time, dine, and go away with; and collective (community), or those with whom you find a sense of a shared identity (5). In his book, he recommends spending 15 minutes per day connecting with someone else with a mindful presence, free of distractions, as one way to combat loneliness.
Other suggestions to battle loneliness for individuals or organizations are:
| Individuals | Organizations |
|---|---|
| Find a buddy to check in with regularly. | Examine the culture—ask about loneliness, connectivity. |
| Work in teams. | Educate leaders about loneliness. |
| Build mentoring relationships. | Connect new hires early, even before they start. |
| Don't eat alone. | Encourage mentoring and buddy programs. |
| Take breaks, and talk to someone! | Engage in frequent team-building activities. |
| Be present when connecting with others. | Sponsor lunches with no agenda. |
| Share with and listen to others. | Talk about loneliness; normalize it. |
| Perform random acts of kindness. | Look out for people who are isolating. |
| Express gratitude. | Build social/connectivity time into meetings; lead by example, and share! |
| Check on someone. | Wherever possible, give the team a say in decision making that affects them. |
Another component to consider in connecting people with each other at work is that we have become a bit socially awkward as a nation! We aren't used to being in close contact with each other and having unmasked or in-person conversations. In addition, for some, there may not be a ton to talk about if life is a bit mundane. Getting people talking through a team-building or connectivity exercise is a useful tool to get over that hump! I designed this exercise to get people talking and also to help them start to consider what good days look and feel like. In doing so, we can empower people to be active contributors to their well-being by building supportive environments and connections. Try it out, and let me know how it goes!
More Good Days
- Make time to pause and think about what is going well, what contributes to good days, and how to build more of that into our days.
- The goal is to have more good days and to know what good days look like for us.
- Identify tangible components of our days that contribute to our well-being.
- Build a sense of control, self-efficacy, and self-advocacy to construct environments in and outside of work that are supportive and sustainable.
What makes for a good day?
- What makes for a good day at work these days?
- What makes for a good day outside of work these days?
- Be specific! What about these things makes you feel good?
How do we get more of the good?
- What would it take to have more of that in each day?
- What do you need to have more good days?
- What can you tell yourself on the tougher days?
Next Steps
- Based on this, what do you want to ask for? This could be of yourself, of someone else, etc.
- What commitment are you ready to make?
References
- Vantage Circle. Workplace loneliness—the silent killer of your organization. 11 February 2019. Accessed at https://blog.vantagecircle.com/workplace-loneliness/amp.
- MindTools. 8 ways to beat loneliness in the workplace. 2021. Accessed at www.mindtools.com/pages/article/loneliness-at-work.htm.
- Cigna. Loneliness is at epidemic levels in America. 2021. Accessed at www.cigna.com/about-us/newsroom/studies-and-reports/combatting-loneliness.
- AARP. How lonely are you? 24 September 2010. Accessed at www.aarp.org/personal-growth/transitions/info-09-2010/How-Lonely-are-You.html.
- Murthy VH. Together: The Healing Power of Human Connection in a Sometimes Lonely World. HarperCollins; 2020.
Want to be featured in our newsletter? Share your success stories and those of inspirational colleagues (both ACP Champions and partners) by e-mailing acpwellbeing@acponline.org.